- EHR and EMR Origins
- Historical Background
- Defining the Terms
- What Is EMR?
- What Is EHR?
- Clearing Up the Confusion
Table of Contents:
Although the acronyms EHR and EMR seem strikingly similar, EMRs were the predecessors, focused solely on digitizing medical records for diagnostic and treatment purposes within a single health provider unit. In contrast, EHRs take electronic recording a step further, as it involves the more comprehensive capture of a patient's overall health data.
For the most part, every healthcare professional today deals with an EHR. This is because its scope covers patient information, care coordination across healthcare providers and facilities, patient engagement, compliance with treatment plans, data sharing capabilities, and ultimately the overall quality of care delivered.
Electronic record systems have been in use since the 20th century, and they have evolved and undergone continuous refinement since then. Despite their long-standing adoption, people still find it ambiguous and puzzling to define and distinguish the terms.
Given these concerns, it’s worth asking: What are the differences between EMR and EHR?
Is there any difference at all?
To address the confusion, let’s first explore their origin.
EHR and EMR Origins
Because of their unclear definitions, some medical specialists use the EMR and EHR interchangeably. Others, well-grounded on the distinction, apply them as separate concepts. The EMR was created for administrative and clinical interactions between providers and patients. It often reflects the healthcare provider’s practice style, skills, knowledge, and job function. This is because EMRs contain data structures and elements specific to the systems designed by their creators.
To standardize the record collection process, the Institute of Medicine (IOM) defined the basic functions of an EMR. This system is also referred to as computerized patient record (CPR), which is considered the definitive gold standard.
In addition to the provider-generated data in the EMR, patients maintain a personal health record (PHR) with electronic copies of information from various healthcare providers.
On the other hand, EHRs were developed to integrate the EMRs generated by numerous physicians with the patient’s PHR. This comprehensive approach of record keeping aims to optimize personal and community health management. EHRs make it possible to share patient data among authorized care providers efficiently.
Additionally, patients are reserved the benefit of approaching any healthcare facility for consultation after authorizing the providers to access their complete health records. The secure Internet connection in EHR fosters the seamless integration of medical information, which benefits provider and patient education.
The development of EHRs wasn't a sudden invention; it was built upon the foundation of EMRs. The concept and context of the terms evolved with time. To learn more about this evolution, we must go back in history.
Historical Background
In the order of things, EMRs clearly emerged first, paving the way for the development of an all-inclusive EHR system as the Internet and technology rapidly advanced. To illustrate the progression, we’ve created a short timeline highlighting the crucial steps along the way.
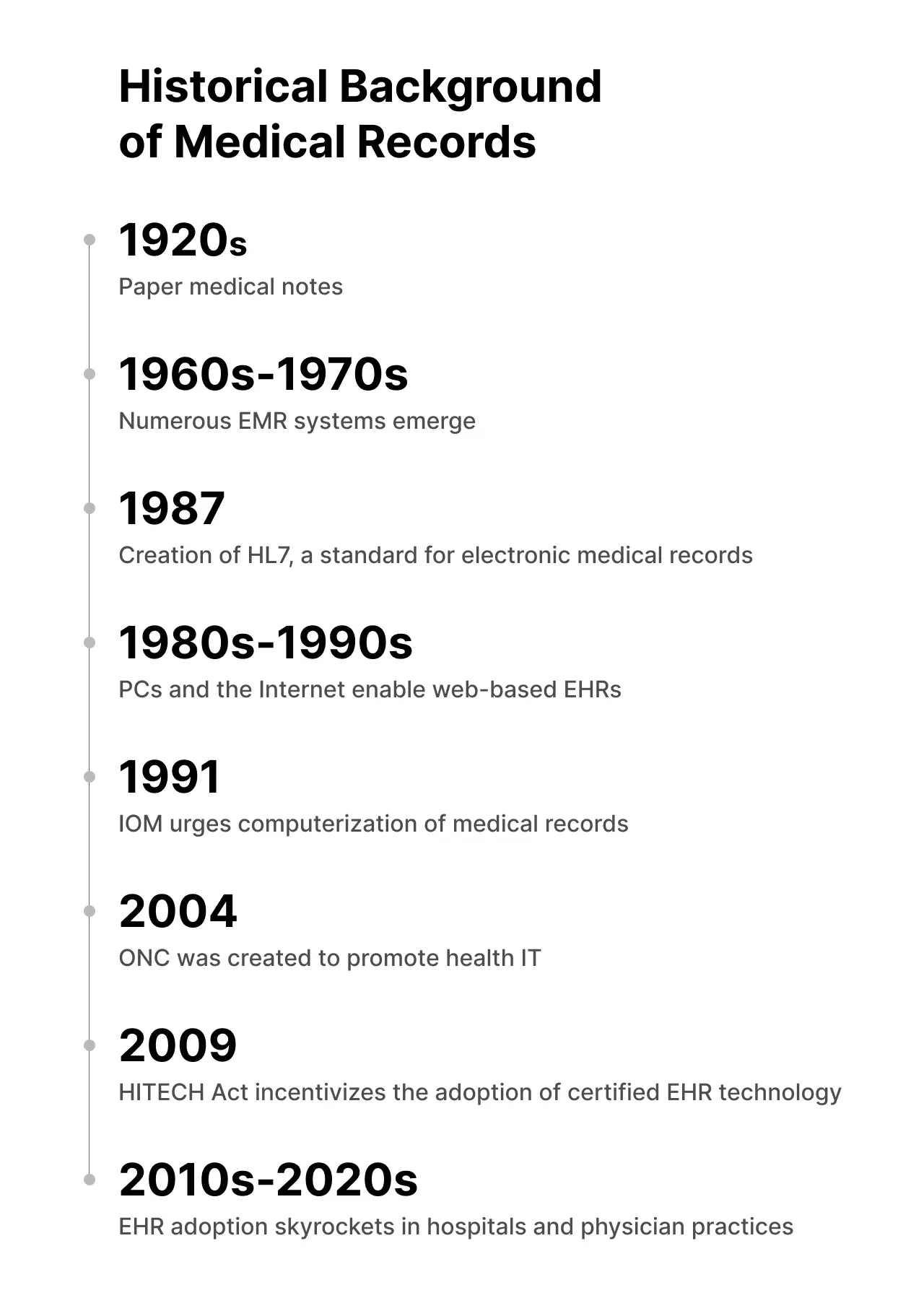
1920s: Medical notes were mostly kept on paper.
1960s-1970s: First EMR systems (POMR, COSTAR, VA MUMPS, TMIS, PROMIS) were created. They were characterized by integrations with scheduling, clinical, and billing systems.
1987: The IOM helped in the collaborative project to create the international non-profit Standards-Developing Organization (SDO), HL7, which develops and maintains standards for electronic data capture, ensuring that all EMR components communicate seamlessly for a comprehensive record system.
The 1980s-1990s: the advancement of hardware, development of personal computers, and rise of the Internet renewed interest in EMRs. Despite the slow speed of the Internet and the memory limitations of computers, these devices could handle clinical tasks. Internet integration allowed for faster information retrieval, leading to the emergence of web-based EHRs.
1991: Through funded studies and papers, the IOM pushed for computerizing patient records. Based on the recommendations, every doctor’s office should have had an EHR by 2000.
2004: President Bush set a goal for most Americans to have EHRs by 2014. Eventually, the Office of the National Coordinator for Health Information Technology (ONC) was inaugurated, and health information technology was adopted.
2009: As part of the HITECH Act, President Obama included EHR in the American Recovery and Reinvestment Act, providing monetary incentives to companies that adopt the meaningful use of certified EHR technologies to promote interoperability.
2010s-2020s: The use of EHR skyrockets, as about 96% of non-federal acute care hospitals and 78% of office-based physicians have adopted the approved EHR.
The rise of electronic recording systems has revolutionized how patient information is captured and stored over the years. This shift begs the question: what do EMR and EHR really stand for?
Defining the Terms
Now, we have explored the historical context of EMRs and EHRs, highlighting how technological innovations have influenced their evolution and applications. With more advancements on the horizon, the question remains:
Can we still use both terms interchangeably or not?
There is actually an answer; you can find it in the National Alliance for Health Information Technology (NAHIT) report, which provides key terms in health information technology. Although NAHIT ceased its operations in 2009, it played a critical role in elevating health IT on a national level.
So, how did it all start?
In 2004, President George W. Bush set an ambitious goal to implement the widespread adoption of EHRs by 2014. This initiative was birthed from the desire to improve healthcare quality, make it possible for everyone to access healthcare, and reduce errors to the barest minimum as well as costs. With proper execution, EHRs are expected to ensure secure health information exchange, support for patient self-management, and research contributions alongside public health efforts and emergency response.
To realize this vision, models capable of interoperability need to be developed, and clear standards in the aspect of data exchange set need to be established. Thus, the NAHIT efforts to facilitate public dialogue further clarified the terminologies and definitions. Now, let’s define the terms.
What Is EMR?
According to the NAHIT report on health IT terminology, an Electronic Medical Record, or EMR, is “an electronic record of health-related information on an individual that can be created, gathered, managed, and consulted by authorized clinicians and staff within one health care organization.”
EMRs are digital versions of traditional paper charts within a single healthcare organization. They allow healthcare providers to easily search and analyze data, improving patient care.
EMRs primarily contain information generated by clinicians to improve documentation processes and treatment. This innovation supports essential functions, including checking for drug interaction and providing well-informed recommendations for better decision-making. However, again, their scope is limited to the data available within a single healthcare entity.
In contrast, an EHR serves a slightly different function.
What Is EHR?
Based on the NAHIPs report, an Electronic Health Record, or EHR, is “an electronic record of health-related information on an individual that conforms to nationally recognized interoperability standards and that can be created, managed, and consulted by authorized clinicians and staff across more than one health care organization.”
EHRs allow various authorized physicians to provide a more seamless approach to maintaining and updating patients' medical records. This recording system has the merit of continuous and sustainable care provision across providers.
By design, EHRs go beyond storing standard clinical data collected at a provider's office. They are an indispensable component of health IT at any medical practice. This is attributed to their accessibility to evidence-based tools and resources, enabling providers to make informed decisions and achieve patient care more effectively.
A key feature of EHRs is their ability to create, manage, and share patient data digitally between authorized providers across various healthcare settings, including specialty clinics, laboratories, pharmacies, and imaging centers. This approach nurtures coordinated care across the facilities involved in patient treatment.
Clearing Up the Confusion
The similarities between EMR and EHR can be quite confusing to many, and it is understandable why healthcare professionals use one instead of the other. However, because they perform the same functions, they are often used interchangeably:
- EMR/EHR has the advantage of providing medical records with just a few clicks to any authorized healthcare professional, whether practice-wide (EMR) or beyond (EHR).
- The systems make things much more efficient by automating specific tasks and cutting down mountainous paperwork. Everything moves faster as providers can see test results, medication lists, and chart notes on the computer.
- Of course, with all that sensitive health data being digitized, security is crucial. EMR/EHR follows all the privacy rules and regulations in the letter.
- Healthcare organizations using either system save tons of money in the long term. No more endless storage rooms of dusty file folders as compact and digital compilations cut those costs.
EHRs represent a more comprehensive and interoperable system. To be clear, the key distinction between EMRs and EHRs lies in this interoperability. EHRs have nationally recognized standards that authorize registered users to share information across various facilities, integrate a broader range of helpful health data, update patient information, and facilitate coordinated care.
To qualify as an EHR, a system must meet specific interoperability standards, which include an understanding of and catering to the following:
- Vocabulary/terminology - CPT, ICD-10 and 11, NDC, etc.
- Content - C-CDA, V2, CDA;
- Transport - DICOM, FHIR, IHE, etc.
- Privacy and security, which we describe in our article about HIPAA;
- Identifiers - NPI, EMPI, OID, etc.
Beyond the benefits both electronic recording systems offer the healthcare industry, the impact of digitization cannot be over-emphasized.
EMRs and EHRs absolutely provide distinct value, whether you're a solo practitioner or part of a massive healthcare network. Remembering their respective functions and leveraging their strengths is crucial for delivering the safest, most efficient patient care possible.